Diabetes is classified into Type 1 diabetes mellitus (TIDM) and Type 2 diabetes mellitus (TIIDM) based on whether the patient has a deficiency in insulin secretion. TIDM is, on the one hand, characterized by destroying pancreatic beta cells that secrete insulin, mainly during childhood and adolescence. On the other hand, TIIDM is characterized by an imbalance between insulin levels and insulin sensitivity, resulting in persistent hyperglycemia. TIIDM is primarily found in middle-aged and elderly individuals. Globally, 90% of diabetes patients have TIIDM. Whether it is TIDM or TIIDM, if patients do not treat their hyperglycemia through appropriate medical interventions, they may face a series of severe consequences like blindness, kidney failure, or amputation.
TIDM primarily requires continuous insulin injections. However, patients with TIIDM have more options. Many traditional small molecule drugs, such as glimepiride, metformin, and acarbose, help to control blood sugar levels. Their main mechanisms include increasing insulin release, enhancing insulin sensitivity, reducing dietary sugar intake, etc. In recent years, with in-depth research on the pancreas and insulin, new approaches have been taken to developing diabetes medications that target GLP-1 receptors and their agonists.
In addition to pancreatic beta cells that secrete insulin, pancreatic alpha cells secrete glucagon in the pancreas. As the name suggests, glucagon can rapidly increase blood sugar levels. Under normal circumstances, glucagon and insulin have a mutual inhibitory and balanced relationship, helping to maintain stable blood sugar levels within an appropriate range. In 1986, Drucker and colleagues made an unexpected discovery while studying the synthesis of the preproglucagon gene (GCG). When glucagon is synthesized in the human body, it first undergoes translation and synthesis by GCG, resulting in a polypeptide called Proglucagon. This peptide chain can be cleaved at different sites to produce various biologically active small peptide segments, one of which becomes glucagon. However, like a long and beautiful necklace that can be cut into several pieces to become different jewelry pieces such as bracelets, earrings, or rings, Proglucagon is also cleaved into multiple products. Among these products, one segment caught the attention of Drucker and colleagues. They named it glucagon-like peptide 1 (GLP-1). Although GLP-1 and glucagon share the same origin, their effects are complete opposites. GLP-1 can promote insulin release in the body, lowering blood sugar levels.
Upon its discovery, GLP-1 immediately sparked great interest among drug developers as it showed tremendous potential to be developed as a novel antidiabetic medication. Further research has also confirmed this. Compared with traditional small molecule antidiabetic drugs, peptide-based drugs modified from GLP-1 have a glucose concentration-dependent effect on stimulating insulin secretion. For patients with TIIDM who do not respond well to sulfonylureas, continuous intravenous infusion of GLP-1 significantly lowers blood glucose levels. However, once blood glucose reaches normal levels, continued administration of GLP-1 does not further stimulate insulin secretion, and blood glucose remains stable. Therefore, GLP-1 analogs carry a low risk of hypoglycemia while regulating blood sugar, making them safer for users. Additionally, GLP-1 may also have the potential to reduce weight and improve pancreatic beta cell function, offering multifaceted regulation of metabolic abnormalities in patients with TIIDM.
GLP-1 analog drugs have become a research hotspot for treating related diseases in TIIDM. Searching for GLP-1 on the North American Clinical Trials Registry yields approximately 2,600 clinical research records. Currently approved GLP-1 analog drugs include Exenatide, Liraglutide, Semaglutide, Dulaglutide, etc. Semaglutide has become the first orally administered GLP-1 antidiabetic drug.
Bioanalysis of GLP-1 Analog Drugs in Clinical Pharmacokinetic (PK) Studies
For the bioanalysis of GLP-1 analog drugs in clinical PK samples, like other peptide/protein drugs, two commonly used methods are ligand binding assay (LBA) and liquid chromatography-mass spectrometry (LC-MS/MS). Each method has its characteristics, as shown in Table 1. Based on the design of different clinical trial protocols, appropriate analytical methods can be chosen to obtain drug concentration information in subjects’ blood.
| LBA | LC-MS/MS | |
| Detection method | Indirect | Direct |
| Sensitivity | pg/mL | μg/mL, ng/mL |
| Throughput | Highest | High |
| Quantitative range | 1-2 orders of magnitude | 3-4 orders of magnitude |
| Selectivity | Moderate | High |
| Method development | Time-consuming | Quick |
| Method transfer difficulty | Dependent on critical reagents | Easy |
LC-MS/MS Method Supports PK Studies of GLP-1 Analog Drugs
Due to the relatively small molecular weight of GLP-1 analog drugs, LC-MS/MS-based assays exhibiting high selectivity and wide linear range are widely applicable in the bioanalysis of GLP-1 analog drugs. It is available for global joint submissions in clinical research. With increasing clinical studies on GLP-1 analog drugs, the bioanalytical methods for PK studies using the LC-MS/MS platform are becoming more mature.
There are two main challenges in quantitatively detecting GLP-1 analog drugs in human blood samples using the LC-MS/MS platform. First, compared to the LC-MS/MS bioanalytical methods for small molecule drugs, the sample preparation process for peptide/protein drugs is often more complex. A combination of protein precipitation (PPT), solid-phase extraction (SPE), and immunocapture methods may be required for adsorption and purification to improve selectivity. The complex sample preparation process poses higher requirements for bioanalytical laboratories, making such projects highly dependent on method reproducibility, operator proficiency and accumulated laboratory experience.
Furthermore, many GLP-1 analog drugs undergo modifications in their structure. Natural GLP-1 is easily degraded by enzymes with a short half-life of only 2-5 minutes, making it unavailable for direct therapeutic use. However, for diabetes treatment purposes, these drugs must have a prolonged duration of action. Therefore, modifications and alterations toward GLP-1 analog peptides are necessary during drug development. In addition to amino acid residue substitutions, structural modifications that extend the half-life are incorporated. For example, liraglutide, a GLP-1 analog, is resistant to the action of dipeptidyl peptidase IV (DPP IV). It has a 16-carbon acyl chain attached to the lysine residue. Lysine at position 34 of GLP-1 is replaced by arginine. This modification allows liraglutide to bind to serum albumin in the plasma, enhancing its sustained-release effect.
Adding long alkane chains makes these drugs more sticky than ordinary peptide/protein drugs, making it extremely easy to cause adsorption and residue in the LC-MS/MS system. Therefore, the LC-MS/MS method for GLP-1 analogs analysis is also special.
LBA Method Supports PK Studies of GLP-1 Analog Drugs Due to the size of the molecules, LBA methods are often more challenging to apply in PK studies of GLP-1 analog drugs than LC-MS/MS methods. However, if specific antibodies are available, corresponding LBA methods can be developed. Figure 1 provides an example of an LBA method developed on the MSD platform for quantifying exenatide in human plasma. This is a typical sandwich assay using biotinylated anti-GLP-1 specific antibody as the capture antibody coated on a 96-well MSD plate. A Ruthenium-labeled anti-GLP-1 specific antibody is used as the detection antibody. To eliminate interference and improve selectivity, sample extraction with a PEG solution is performed prior to sample loading. Compared to LC-MS/MS methods, LBA method development often takes longer. But it typically offers higher sensitivity. The detection limit can reach the pg/mL level if highly specific antibodies are available. Additionally, the high throughput of LBA makes it widely applicable in clinical PK studies.
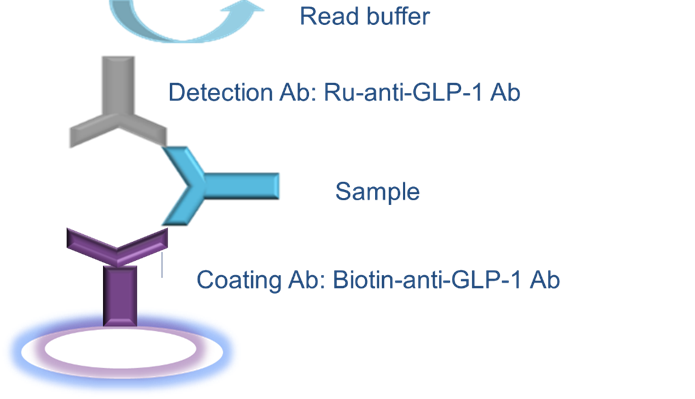
Figure 1. Example of an LBA method based on the MSD platform
Scientists have also discovered that linking the GLP-1 peptide chain to an Fc-fusion protein fragment can further increase the half-life, leading to the development of dulaglutide. Compared to liraglutide, dulaglutide, with the addition of the Fc-fusion protein structure, has a significantly increased molecular weight that may reach 60 kDa. This allows it to effectively avoid degradation by lysosomes and greatly extend the half-life. Indirect LBA methods have advantages in clinical PK detection for such drugs with larger molecular weights.
Biological Analysis of Drug Immunogenicity of GLP-1 Analogs
Like other biologics, patients receiving GLP-1 analog drugs may develop corresponding anti-drug antibodies (ADAs) and neutralizing antibodies (NAbs) in their bodies. Since immunogenicity strongly correlates with drug effectiveness and safety, regulatory authorities require immunogenicity assessment for all biological drugs. Immunogenicity testing for GLP-1 analog drugs can be done using methods such as electrochemiluminescence (ECL) and radioimmunoassay (RIA).
Bridging assay on the MSD platform supports the study of anti-drug antibodies (ADAs) for GLP-1 analog drugs. It has the characteristics of high sensitivity, widely effective linear range, high homogeneity, high reproducibility, minimal matrix effect, good stability and high detection throughput. This assay is widely used for immunogenicity testing of GLP-1 analog drugs.
GLP-1 analog drugs have relatively smaller molecular weights compared to larger biologics. Biotin and ruthenium labeling efficiencies are lower for smaller molecules. During the method development stage, the drug’s characteristics must be considered. A more complex but higher labeling efficiency labeling method, such as the dialysis membrane method or direct chemical synthesis, must be chosen.
If GLP-1 analog drugs are being submitted as biosimilars, they also require a comparability assessment with the reference drug, including threshold evaluations and examination of parameters such as drug tolerance. The comprehensiveness and completeness of the evaluation rely on a thorough interpretation of guidance principles and accumulated verification experience.
Radioimmunoassay (RIA) is a highly sensitive analytical technique used to measure minute quantities of non-labeled antigens. It involves the competitive binding of labeled and non-labeled antigens to their specific antibodies, allowing sufficient time for the reaction to reach equilibrium. The resulting antigen-antibody complexes are then separated, and their radioactivity is measured using an automated gamma counter. The radioactive counts of the bound antigen-antibody complexes and the free antigen are used to calculate the concentration of the non-labeled antigen.
The RIA method has high sensitivity, strong specificity, and good precision and stability. For example, GLP-1 analog drugs like Semaglutide can be tested for immunogenicity using the classical radioimmunoassay (RIA) method, which can better meet the requirements of global joint submissions for method consistency in clinical research.
A Cell Platform is Recommended for Neutralizing Antibody (Nab) Detection of GLP-1 Analogs
The first method is based on the competitive homogeneous time-resolved fluorescence (HTRF) detection of the cyclic adenosine monophosphate (cAMP) signaling pathway mediated by GS protein. HTRF technology relies on fluorescence resonance energy transfer (FRET) and time-resolved fluorescence (TRF). Energy transfer occurs when cAMP labeled with HTRF acceptor d2 (cAMP-d2) and the anti-cAMP antibody labeled with europium (Eu) as the energy donor (Anti-cAMP-Cryptate) are in proximity, resulting in the generation of fluorescence signal.
In specific cell lines expressing recombinant human GLP-1 receptors, the action of GLP-1 analogs can stimulate the expression of intracellular cAMP. This competes with the binding of the anti-cAMP antibody labeled with europium (Eu) as the energy acceptor to the cAMP-d2. Therefore, the fluorescence signal is inversely proportional to the intracellular cAMP level and positively correlated with the amount of neutralizing antibody.
The second method of neutralizing antibodies (NAb) detection is to use the firefly luciferase gene expression as a reporter gene. Recombinant HEK293 cells stably expressing GLP-1R and controlled by the cAMP expression of the firefly luciferase gene are used. Under the action of GLP-1 analogs, the protein kinase A signaling pathway is activated, which promotes the expression of the intracellular luciferase gene. In the presence of neutralizing antibodies, the binding of GLP-1 to GLP-1R is blocked, resulting in a decrease in the fluorescence signal.
A Final Word
GLP-1 antagonist drugs have emerged as a novel therapeutic option for TIIDM. Unlike traditional antidiabetic drugs, GLP-1 analogs leverage the peptide’s ability to stimulate insulin release while minimizing hypoglycemia risk. With advances in drug development, these peptides are modified to enhance their stability and efficacy, such as extending their half-life or improving their resistance to enzymatic degradation. Two major analytical methods – LBA and LC-MS/MS – are used for PK studies, each with strengths and challenges. Immunogenicity assessments, including the detection of anti-drug antibodies and neutralizing antibodies, are essential for ensuring drug safety and effectiveness.
As a global company with operations across Asia, Europe, and North America, WuXi AppTec provides a broad portfolio of R&D and manufacturing services that enable the global pharmaceutical and life sciences industry to advance discoveries and deliver groundbreaking treatments to patients. Through its unique business models, WuXi AppTec’s integrated, end-to-end services include chemistry drug CRDMO (Contract Research, Development and Manufacturing Organization), biology discovery, preclinical testing and clinical research services, helping customers improve the productivity of advancing healthcare products through cost-effective and efficient solutions. WuXi AppTec received an AA ESG rating from MSCI for the fourth consecutive year in 2024 and its open-access platform is enabling around 6,000 customers from over 30 countries to improve the health of those in need – and to realize the vision that “every drug can be made and every disease can be treated.”